This post is an update on my experiment testing whether inspiratory muscle training reduces my blood pressure. Below is an interim analysis of the first 3 weeks of the 6 week, pre-registered experiment. So far, I’m seeing a large improvement in inspiratory muscle strength, but no effect on blood pressure. Not looking good, but hopefully I’ll start seeing an effect on blood pressure in the next few weeks.
Summary
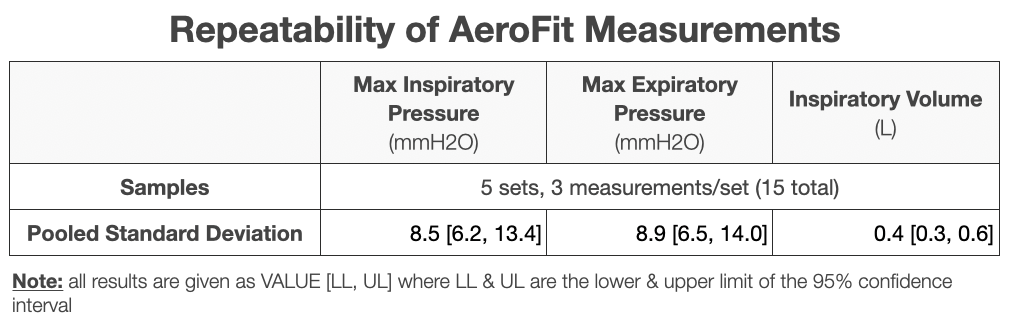
Measurement Precision:
The Aerofit shows sufficient precision for measuring inspiratory volume and maximum inspiratory & expiratory pressure (see Table below), with a standard deviation < the week-to-week improvement.
Strength Improvement:
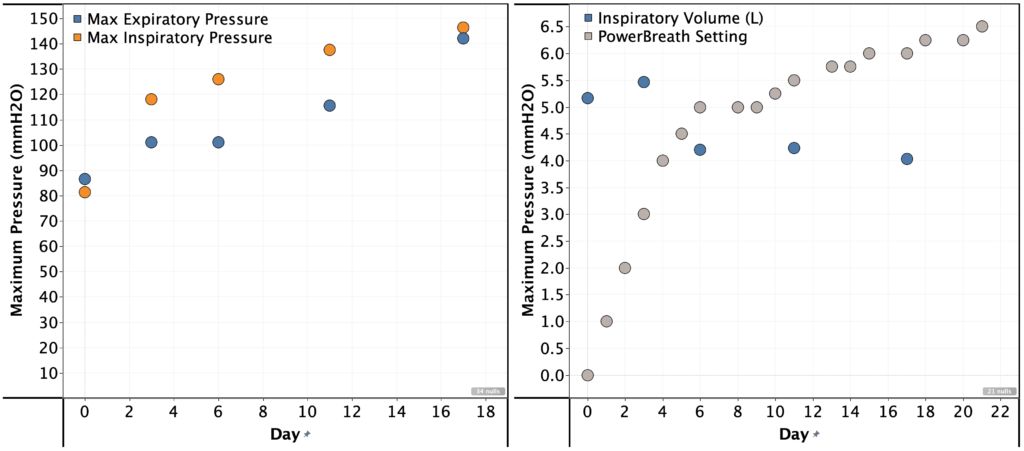
I was able to significantly increase the resistance setting on the PowerBreath. In week 1, I couldn’t complete the full set of breaths at setting 5. By week 3, I could do so for setting 6.25.
This correlated with a large increase maximum inspiratory & expiratory pressure, but a reduction in inspiratory volume.
Maximum inspiratory pressure: 81 -> 146 mmH2O
Maximum expiratory pressure: 87 -> 142 mmH2O
Maximum inspiratory volume: 5.2 -> 4.0 L
Blood Pressure:
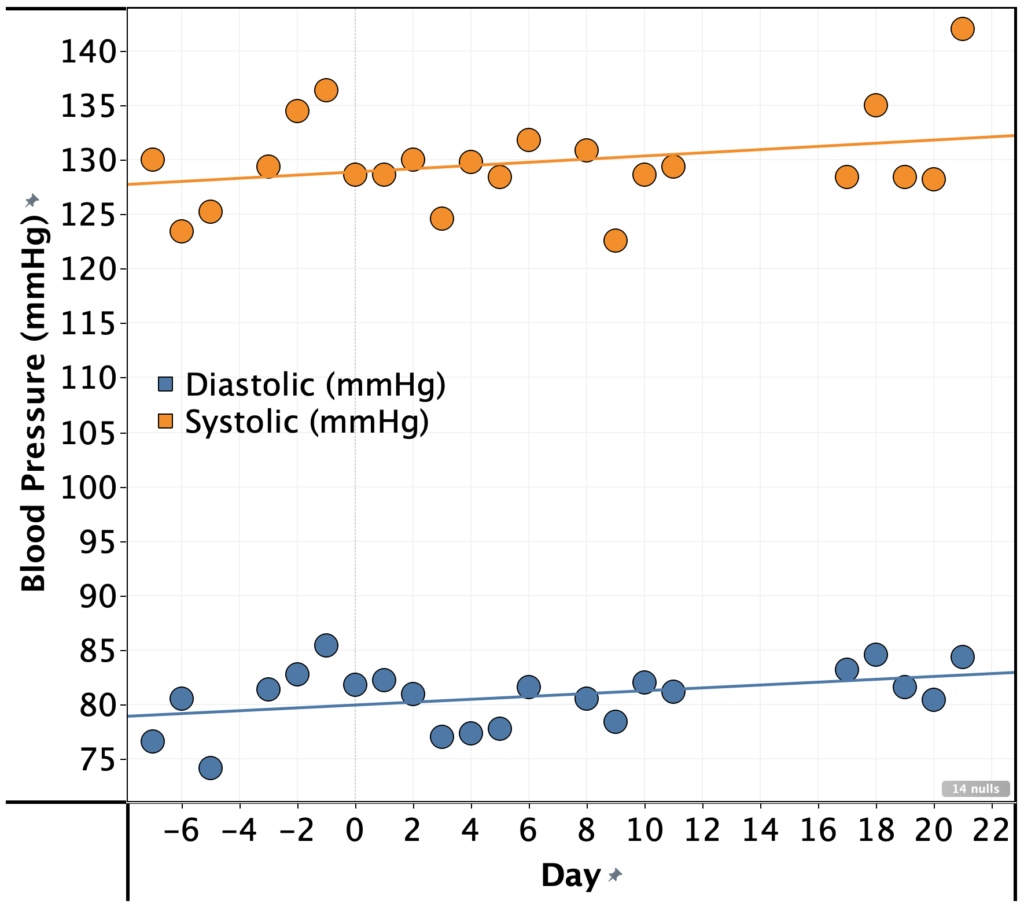
Despite the large improvement in inspiratory muscle strength, I’ve seen a no improvement in my blood pressure in the first 3 weeks. In fact, it’s gotten slightly worse (see graph).
Systolic: 130 -> 132 mmHg
Diastolic: 80 -> 84 mmHg
Conclusions & Next Steps:
The experiment was pre-registered for 6 weeks, so I will complete the remaining 3 weeks and a full analysis of the results.
I increased the PowerBreath setting by 1 unit per day until I was unable to maintain full pressure for all 5 sets. After that, I followed the pre-registered protocol of increasing by 0.25 when I was able to complete all 5 sets without struggle.
Reason: the lowest settings were way too easy and I wanted to get to a setting that would be a challenge more quickly.
AeroFit measurements frequency varies from the planned frequency of every 3 days.
Reason: I sometimes forgot.
Blinding
This experiment was not blinded
Procedure
Once per day, I did 5 sets of 6 breaths, with 1 min. rest in-between sets using the PowerBreathe HR.
If I struggled to complete all sets, I left the load setting as-is. If not, I increased by 0.25 turns of the load setting knob.
Every 3-5 days, I measured my maximum inspiratory pressure, expiratory pressure, and inspiratory volume using an Aerofit Pro.
Each morning at ~6am, I measured my blood pressure and pulse using an Omron Evolve
Measurements
Blood Pressure
Instrument: Omron Evolve blood pressure meter
Method:
For each measurement, I placed the meter on my left arm, ~4 cm above my elbow.
Measurements were taken seated, with my feet on the ground and arms resting on a flat surface at a comfortable height (same every time).
5 measurements were taken with no pause in-between measurements (other than to write down the result) and the average of the 5 measurements was used.
Breathing:
Instrument: AeroFit Pro
Method:
Following the instruction in the AeroFit app
3 measurements were taken with no pause in-between measurements (other than to write down the result) and the average of the 3 measurements was used.
On a previous post in my blood pressure series, u/OrganicTransistor suggested trying to strengthen my respiratory muscles based on the results in this paper by Seals and co-workers.
The paper, the authors report a pre-registered, sham-controlled, double-blind RCT of whether inspiratory muscle strength training lowers blood pressure. Here’s a quick summary:
36 participants, all with blood pressure >120 mmHg systolic and no indication of uncontrolled diabetes, cholesterol, or thyroid disease or severe obesity.
Participants underwent 6 weeks of IMST using a PowerBreathe K3
Each week, the experimenters measured the participants max inspiratory pressure
The experimental group trained daily at 75% of max inspiratory pressure (5 sets of 6 breaths with 1 min. rest in-between)
The control group trained at very low resistance.
Results:
Systolic: experimental group saw a decrease of 9 mmHg systolic vs. 3 mmHg systolic for the sham-training group (P < 0.01 for difference of means).
Diastolic: experimental group saw a decrease of 2 mmHg systolic vs. 0 mmHg systolic for the sham-training group (P = 0.03 for difference of means).
Results were similar in magnitude and statistically significant when stratified by sex.
Effect persisted 6 weeks after training was stopped.
This is a huge effect size for blood pressure reduction. Given that it was pre-registered, blinded, and sham-controlled, I think it’s worth trying to see if it works for me.
Towards that end, I’m pre-registering the following self experiment:
Approach
I will replicate the published procedure as much as possible, with the following changes:
Instead of a PowerBreathe K3, I will use a PowerBreathe HR for training and an AeroFit Pro for measuring my progress
Reason: The K3 is ~$500, out of my price range for an initial replication
Instead of setting the resistance to a percentage of my max inspiratory pressure, I will increase the load until it is difficult to maintain steady, high pressure for the full 5 sets. Then I will increase by 0.25 turns of the load setting knob whenever I feel able to do so.
Reason: The HR does not have the ability to set a specific load force. The procedure I’m using is the one recommended for training in the PowerBreath HR manual
Procedure
Once per day, I will do 5 sets of 6 breaths, with 1 min. rest in-between sets using the PowerBreathe HR.
If I struggle to complete all sets, I will leave the load setting as-is. If not, I will increase by 0.25 turns of the load setting knob.
Every 3 days, I will measure my maximum inspiratory pressure, expiratory pressure, and inspiratory volume using an Aerofit Pro
Each morning at ~6am, I will measure my blood pressure and pulse using an Omron Evolve
Measurements
Blood pressure:
Instrument: Omron Evolve blood pressure meter
Method:
For each measurement, I will place the meter on my left arm, ~4 cm above my elbow. Measurements will be taken seated, with my feet on the ground and arms resting on a flat surface at a comfortable height (same every time).
5 measurements will be taken with no pause in-between measurements (other than to write down the result) and the average of the 5 measurements will be used.
Breathing:
Instrument: AeroFit Pro
Method:
I will follow the instructions provided by the AeroFit app
3 measurements will be taken with no pause in-between measurements (other than to write down the result) and the average of the 3 measurements will be used.
Analysis
Primary endpoints will be systolic and diastolic pressure for the week prior to and immediately after 6 weeks of training.
Secondary endpoints will be:
maximum inspiratory pressure, expiratory pressure, and inspiratory volume, and pulse for the week prior to and immediately after 6 weeks of training.
All primary and secondary endpoints every two weeks during training
If any significant effects are observed, I will continue tracking for an additional 6 weeks to see if the effect persists.
Effects will be considered of significant magnitude if a reduction of at least 3 mmHg is observed with a p-value of < 0.05.
These experiments started ~1 week ago, though I haven’t looked at the data. I expect to have the first interim analysis in 2 weeks and the full study results in 7 weeks.
This is an update on my experiments to determine the cause and methods to reduce my elevated blood pressure. In this post, I take a look at the correlations between blood pressure and my other self-tracking metrics.
I didn’t find any large or actionable effects, but I’m concerned that the statistical analysis I did was too simplistic or otherwise not correct.
If anyone is interested in taking a look at the data, let me know. All the raw data is provided below, but I’m happy to do additional data processing/cleaning if it would be helpful.
Summary
Background:
I’ve been measuring blood pressure, sleep, weight, hemoglobin, and cholesterol for the past 6 months.
This provides a (hopefully) rich dataset for identifying environmental or lifestyle factors that influence my blood pressure.
Notably, I observed that my blood pressure seems elevated on days after after I’ve had low blood sugar the night before, indicating a possible effect (no statistical or other rigorous analysis done)
Approach:
6 months of self tracking data was aggregated and cleaned.
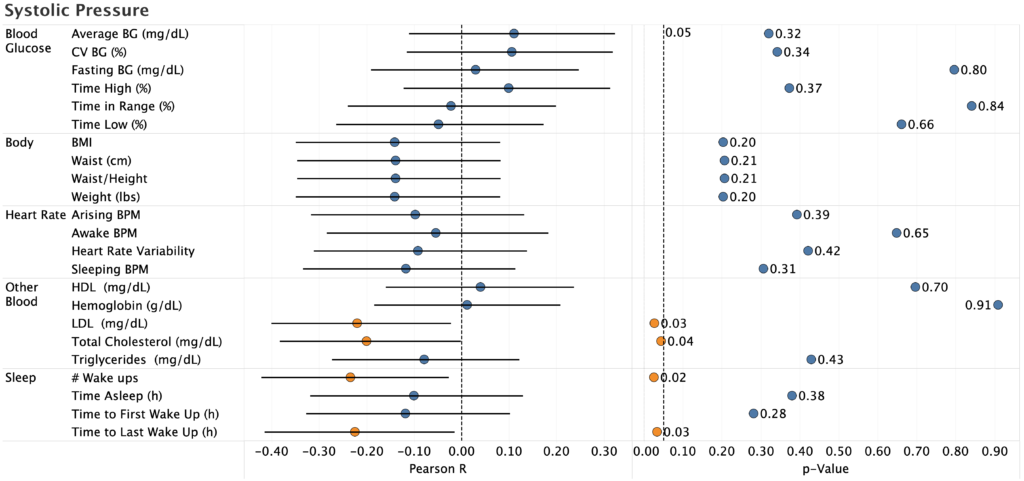
Pearson R and p-value were calculated for 26 metrics that seemed most likely to influence blood pressure compared with systolic pressure, diastolic pressure, and pulse.
Results & Conclusions:
No metric had a large & statistically significant correlation with either systolic or diastolic
Sleep had the largest correlation with systolic pressure:
Effect Size: -1.1 mmHg/h asleep
R2 = 0.05
p-value = 0.03
There was a statistically significant correlation between cholesterol and both systolic & diastolic pressure, but it was in an implausible direction (higher cholesterol showed lower blood pressure), so is likely due to a common cause.
Pulse showed a strong correlation with fasting blood glucose. My suspicion is that this is related to the dawn phenomenon (liver dumping glucose into the blood in the morning to provide energy) as the time from waking up to doing my BP measurements may be correlated to both measures.
Effect Size: 0.08 bpm/(mg/dL glucose)
R2 = 0.14
p-value = 0.0005
Pulse also showed a strong correlation with body weight, though this is likely due to increased aerobic exercise during the same time period.
Next Steps:
Given the small effect sizes and lack of statistical significance, unless I screwed up the analysis, I don’t see any reason to follow up on these results.
Instead, I’ll take a look after 3-6 months and see if additional data surfaces anything useful.
Inspiratory muscle training:
u/OrganicTransistor suggested trying strengthening my respiratory muscles based on the results in this paper.
The results look promising, so I’m going to give the protocol in the paper a try.
This study will take six weeks. I’ve currently completed 8 days and will do an interim analysis every two weeks.
Decrease Sodium/Potassium ratio
Sodium/Potassium ratio has been shown to strongly correlate with blood pressure and incidence of heart disease.
Many years ago, my dad has high blood pressure that lowered significantly when he reduced his sodium intake.
I’m going test substituting a large fraction of my added sodium intake with potassium. Experimental details and pre-registration to follow in a separate post.
Details
Purpose
To determine if any of the metrics I track correlate with blood pressure.
I’ve been measuring blood pressure, sleep, weight, hemoglobin, and cholesterol for the past 6 months.
This provides a (hopefully) rich dataset for identifying environmental or lifestyle factors that influence my blood pressure.
Notably, I observed that my blood pressure seems elevated on days after after I’ve had low blood sugar the night before, indicating a possible effect (no statistical or other rigorous analysis done)
Results & Discussion
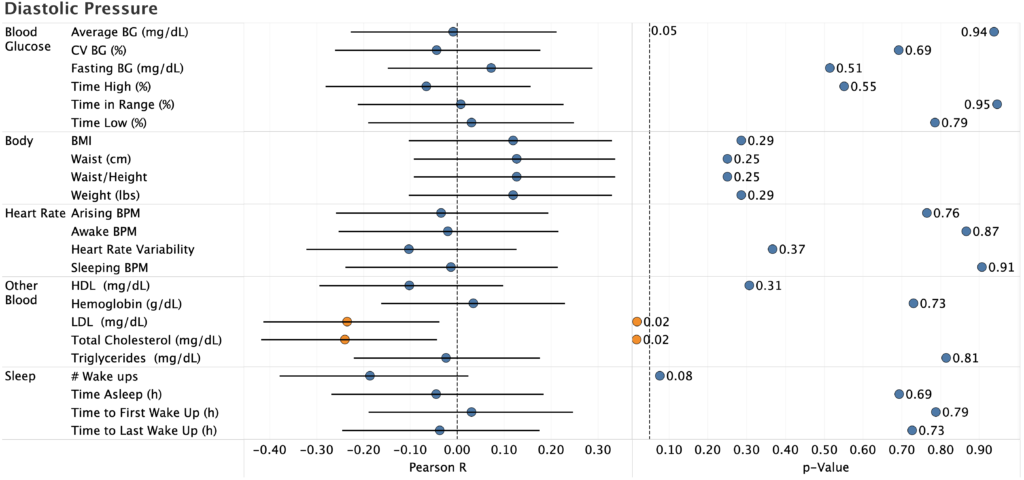
Systolic & Diastolic Pressure
The only statistically significant effects were:
Total cholesterol (systolic and diastolic)
LDL (systolic and diastolic)
# Wake ups (systolic only)
Time to Last Wake Up (manual recording of time asleep, systolic only)
Pearson R is negative for the two cholesterol correlations, which is biologically implausible (there’s no reason high cholesterol would reduce blood pressure). Since I only measure cholesterol once every two weeks, there’s not much data there, so it’s likely a spurious correlation.
For sleep, the correlation is likely real (p=0.03, 95%CI does not overlap zero), but the effect size is to small to be useful:
R2 = 0.05
-1.1 mmHg/h of sleep (i.e. I’d need to sleep an additional 5h to reduce BP by 5 mmHg, which is impossible even if the effect stayed linear)
This gives further evidence to the desirability of keeping my sleep under control, but does not provide a way to meaningfully reduce my blood pressure (I already sleep 6-6.5h/night, so there’s not enough room for improvement).
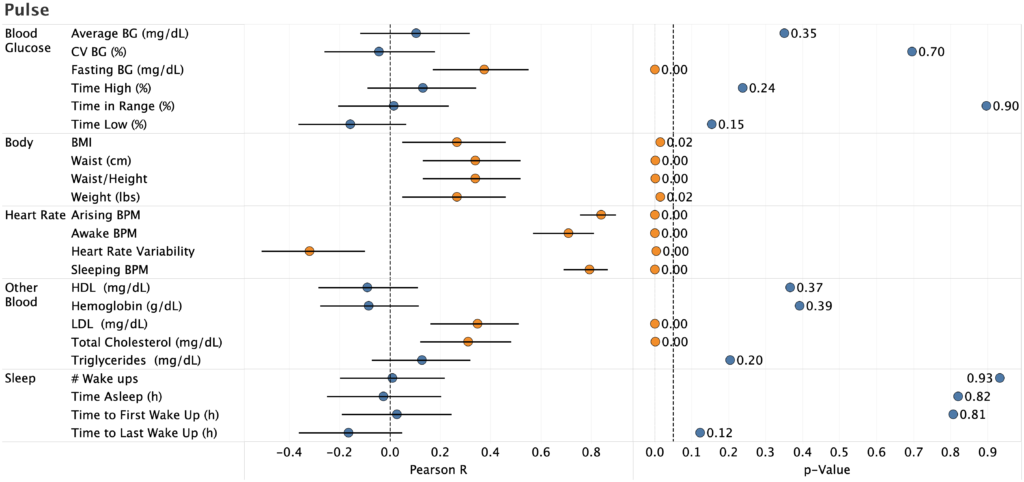
Pulse
Unsurprisingly, pulse strongly correlated with pulse and heart rate variability measured by my Apple Watch. Nice to see, but not actionable.
Strong correlation with fasting blood glucose with a large effect size.
Effect Size: 0.08 bpm/(mg/dL glucose)
R2 = 0.14
p-value = 0.0005
My suspicion is that this is related to the dawn phenomenon (liver dumping glucose into the blood in the morning to provide energy) as the time from waking up to doing my BP measurements may be correlated to both measures. I already work to keep my fasting BG in the normal range for a non-diabetic, so there’s nothing actionable here.
There’s also a strong correlation between pulse and body weight, though this is likely due to increased aerobic exercise during the same time period.
I’m concerned, however, that the statistical analysis I did was too simplistic or otherwise not correct. In particular:
Would a mixed-effect model or other more sophisticated technique surface effects that I can’t detect?
Are there interaction effects that, if accounted for, would provide better predictive value?
Are there other metrics that I missed (e.g. different time lags)?
If anyone is interested in taking a look at the data, let me know. All the raw data is provided below, but I’m happy to do additional data processing/cleaning if it would be helpful.
Absent someone finding an effect I missed, I don’t see any reason to follow up on these results. Instead, I’ll take a look after 3-6 months and see if additional data surfaces anything useful.
In the meantime, I’ll focus on testing additional interventions. Specifically:
Inspiratory muscle training:
u/OrganicTransistor suggested trying strengthening my respiratory muscles based on the results in this paper.
The results look promising, so I’m going to give the protocol in the paper a try.
This study will take six weeks. I’ve currently completed 8 days and will do an interim analysis every two weeks.
Decrease Sodium/Potassium ratio
Sodium/Potassium ratio has been shown to strongly correlate with blood pressure and incidence of heart disease.
Many years ago, my dad has high blood pressure that lowered significantly when he reduced his sodium intake.
I’m going test substituting a large fraction of my added sodium intake with potassium. Experimental details and pre-registration to follow in a separate post.
Instead of a mixed-effect model, I just calculated Pearson R and p-value for each correlation.
Reason: Since there were no effects of a practical/ actionable magnitude, I didn’t spend the effort to figure out how to implement the mixed effect model.
Based on my repeatability study, I’ve repeated the experiment, this time measuring my blood pressure 5 times for each observation. Here’s the result:
Summary
Background:
Numerous studies, reviews, and meta-analyses have shown deep breathing to lower blood pressure in both the short and long-term (example 1, example 2).
Effect sizes are moderate (3-5 mmHg) and statistically significant for large patient populations (>10,000 patients in some studies).
Numerous breathing protocols have been tested, with varying results.
My own tests suggested a possible effect: first, second.
Approach:
Blood pressure and pulse were measured each morning before and after the following protocols:
8s inhale, 8s exhale, 5 min.
Normal activity, 5 min.
For each measurement, I took 5 readings and averaged the results.
Protocols were alternated by day for 10 days (5 days each protocol).
Average and 95% confidence intervals were compared for each metric & protocol.
Results & Conclusions:
With additional, lower variance measurements, I did not observe a meaningful drop in blood pressure or pulse. For all metrics, the difference between deep breathing and normal activity overlapped zero effect and was lower than my target for “clinical” significance.
While the variance is still too large to rule out a clinically significant effect size, it’s sufficiently unlikely that I’m not going to continue testing the short term effect of deep breathing.
Next Steps:
Retrospective analysis of self tracking data
I’ve finished the analysis and just need to write it up for posting.
There were no effects that were practically meaningful and statistically significant, but a few things were worth keeping an eye on.
Inspiratory muscle training:
On my last post u/OrganicTransistor suggested trying strengthening my respiratory muscles based on the results in this paper.
I’m going to replicate their protocol as best I can (pre-registration to follow in another post).
This study will take six weeks, but I will do an interim analysis every two weeks.
Details
Purpose
To determine the effect of deep breathing protocols on short-term blood pressure.
Numerous studies, reviews, and meta-analyses have shown deep breathing to lower blood pressure in both the short and long-term (example 1, example 2).
Effect sizes are moderate (3-5 mmHg) and statistically significant for large patient populations (>10,000 patients in some studies).
Numerous breathing protocols have been tested, with varying results.
My own tests suggested a possible effect: first, second.
Results & Discussion
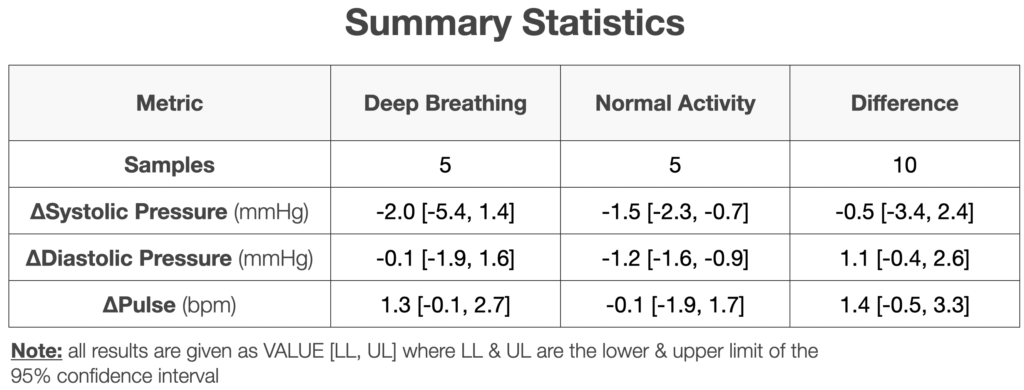
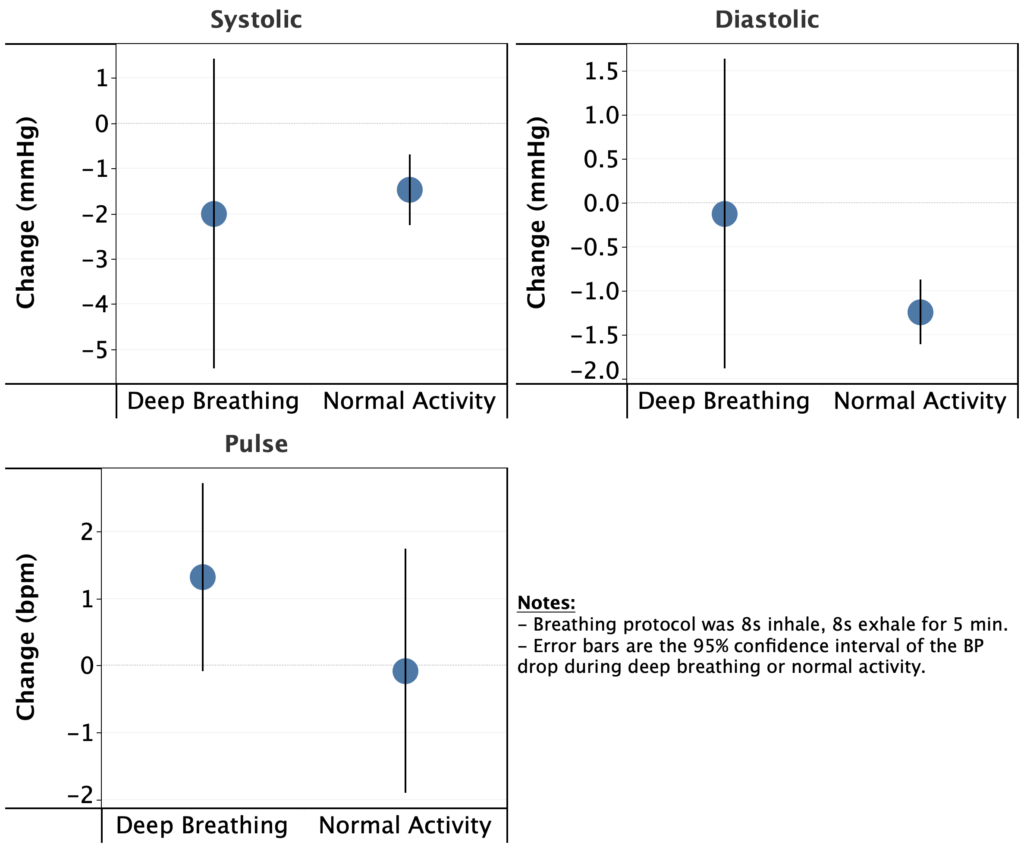
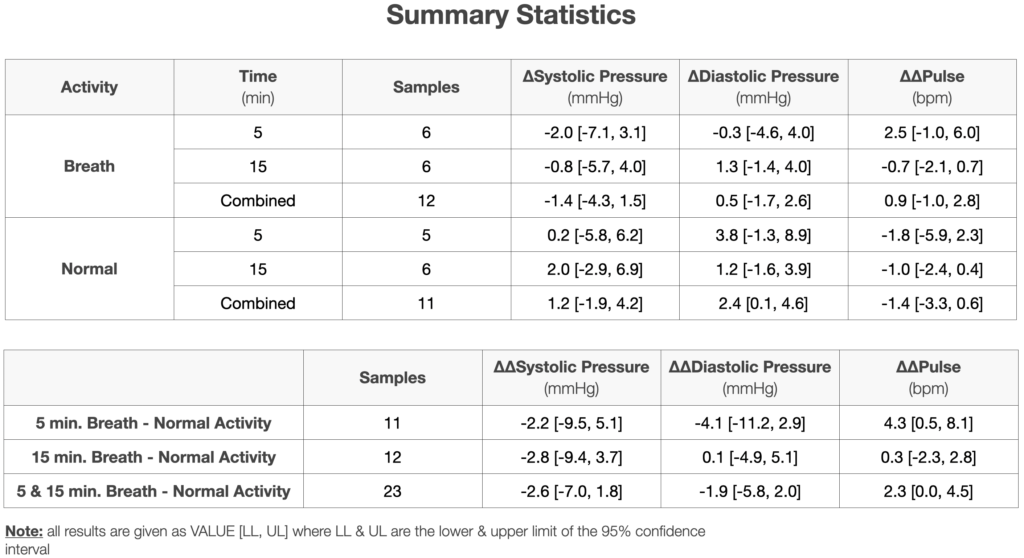
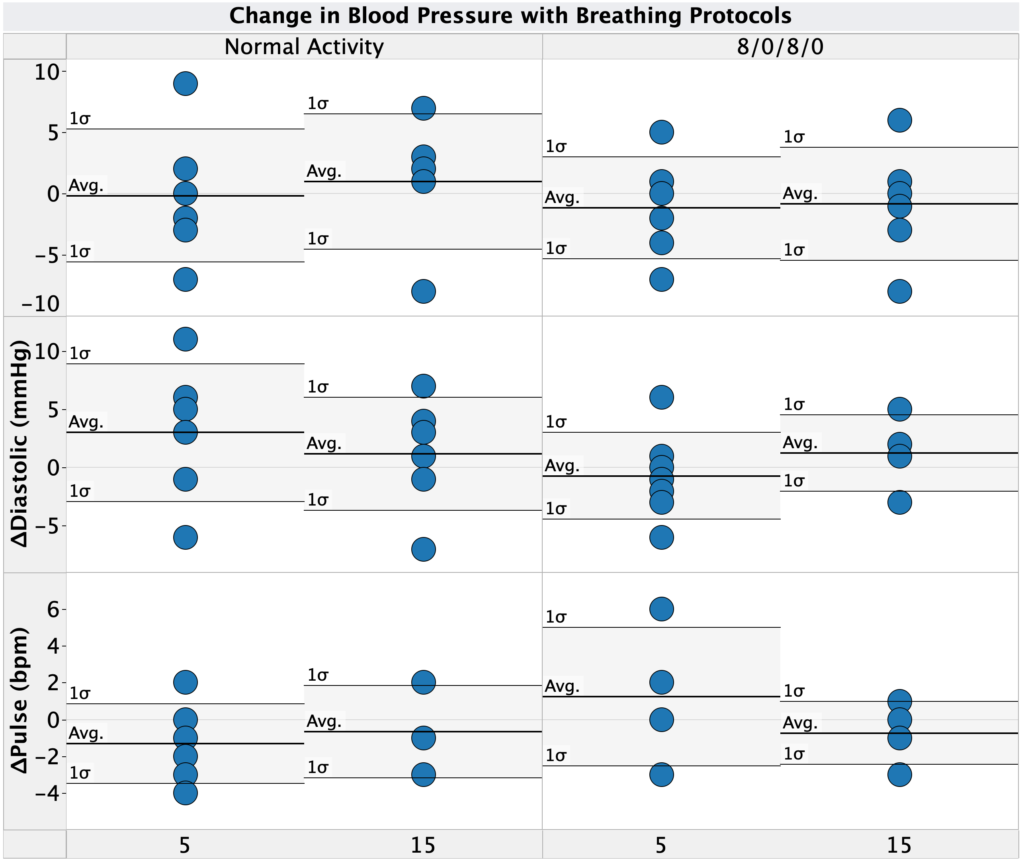
First, let’s take a look at the change in blood pressure for each protocol (deep breathing & normal activity). As shown in both the table and graphs above, on average:
Systolic pressure dropped for both deep breathing and normal activity.
In both cases, the magnitude was modest, 2.0 & 1.5 mmHg for deep breathing and normal activity, respectively.
Since I took these measurements ~1h after waking up, this drop is presumably related to my morning routine in some way (e.g. dissipation of the initial stress from waking up, relaxing during morning computer work, etc.)
Diastolic pressure was nearly unchanged with deep breathing (0.1 mmHg drop), but showed a modest drop for normal activity (1.2 mmHg)
Pulse increased during deep breathing (1.3 bpm) and stayed the same during normal activity (0.1 bpm increase).
Since I took these measurements ~1h after waking up, these effects, if real, are presumably related to my morning routine in some way (e.g. dissipation of the initial stress from waking up, relaxing during morning computer work, etc.)
Several of these effects are different than my previous observations. Notably:
I saw a drop in systolic and diastolic blood pressure in the normal activity condition vs. no change or increase previously.
I saw an increase in pulse in the normal activity condition vs. a decrease previously.
In no case was the difference outside of what would be expected due to the high variance in the previous experiments. As such, the differences are likely due to chance.
Given the much lower variance in the current experiment (5 measurements per condition vs. 1) I have a lot more confidence in the current conclusions.
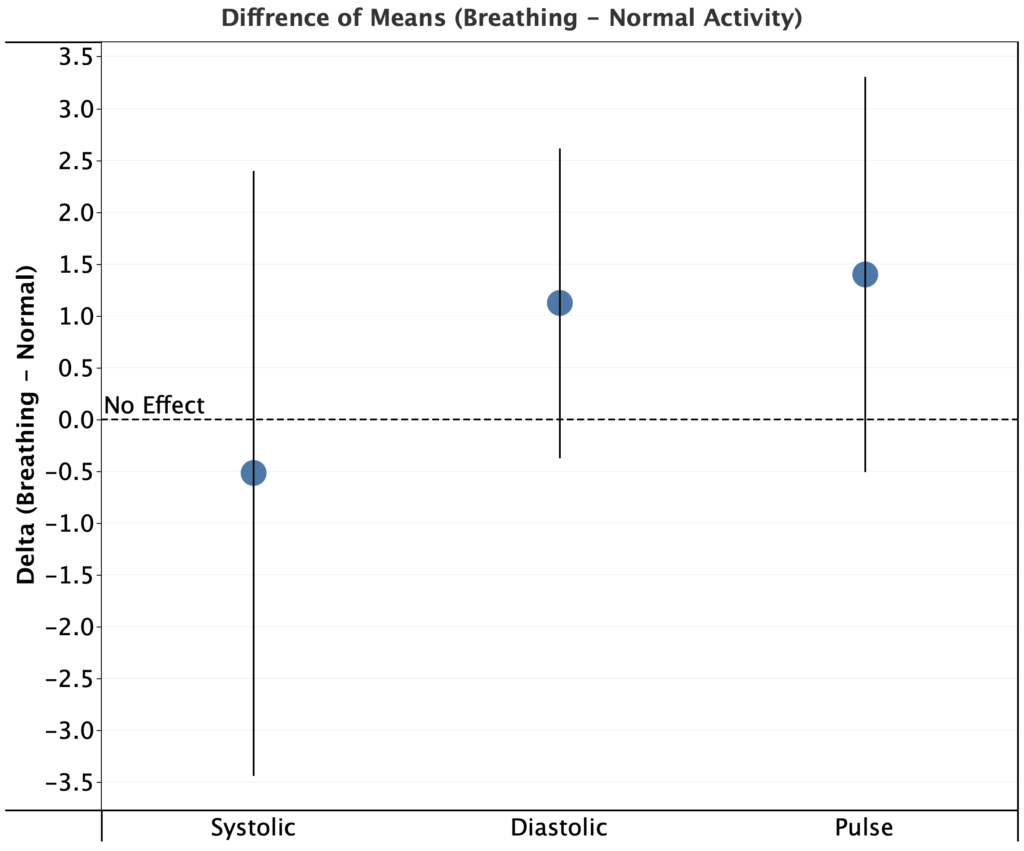
Looking at the difference between means (deep breathing – normal activity) for each metric, I see a decrease of only 0.5 mmHg for systolic pressure, an increase of 1.1 mmHg for diastolic pressure, and an increase of 1.4 bpm for pulse. In all cases, the 95% CI for the difference of means overlaps zero.
Since the measured effects are below my target for “clinical” significance and have a low probability of reaching the target with larger a sample size, it looks like deep breathing doesn’t meaningfully lower my blood pressure.
As mentioned in the background section, there are numerous published studies showing moderate effect sizes (3-5 mmHg) and statistically significant blood pressure drop during deep breathing for large patient populations. While my experiments indicate that this doesn’t work for me, it doesn’t mean the literature is mistaken. Some hypotheses:
Most literature experiments were done in a clinical environment during the day. Due to the environment, the patients might have been more stressed, which can cause an increase in blood pressure and be mitigated by the deep breathing.
My baseline stress may be lower than average and therefore methods to reduce stress (e.g. deep breathing) have a reduced effect on me.
I breath more deeply during normal activity than average.
Other natural person to person variation
This is obviously a catch-all, but in the published studies, it was not the case that every patient showed a drop in blood pressure, just that there was a drop on average.
Conclusions & Next Experiments
It looks like deep breathing doesn’t meaningfully lower my blood pressure. The measured effects are below my target for “clinical” significance and have a low probability of reaching the target with larger a sample size.
Given that I’m not going to continue testing the short term effect of deep breathing on blood pressure. For my next experiments, I’m going to look at the following:
Retrospective analysis of self tracking data
I’ve finished the analysis and just need to write it up for posting. There were no effects that were practically meaningful and statistically significant, but a few things were worth keeping an eye on.
Inspiratory muscle training:
On my last post u/OrganicTransistor suggested trying strengthening my respiratory muscles based on the results in this paper.I’m going to replicate their protocol as best I can (pre-registration to follow in another post).
This study will take six weeks, but I will do an interim analysis every two weeks.
Increasing my Potassium:Sodium ratio
Still figuring out how to test this in a rigorous way. Will pre-register as soon as I work it out.
Instead of using students t-test, I compared 95% confidence intervals between conditions (mathematically equivalent for a threshold of p = 0.05)
Blinding
This experiment was not blinded
Procedure
Each morning at ~6am, I measured my blood pressure before and after the following protocols:
8s inhale, 8s exhale, 5 min.
Normal activity, 5 min.
Breath timing was controlled using the iBreath app.
Blood pressure measurements were performed using an Omron Evolve blood pressure meter.
For each measurement, I placed the meter on my left arm, ~4 cm above my elbow. Measurements were taken seated, with my feet on the ground and arms resting on a flat surface at a comfortable height (same every time).
5 measurements were taking with no pause in-between measurements (other than to write down the result) and the average of the 5 measurements was used.
Blood pressure and pulse were measured each morning before and after the following protocols:
8s inhale, 8s exhale, 5 min.
Normal activity, 5 min.
8s inhale, 8s exhale, 15 min.
Normal activity, 15 min.
Each protocol/time combination was measured 5 times.
Average and 95% confidence intervals were compared for each metric & protocol.
Results & Conclusions:
For each time condition, a blood pressure drop was observed on average during deep breathing, while an increase was observed during normal activity. The opposite effect was observed for pulse (increased during deep breathing).
Due to the high variance in the measurements, the 95% confidence interval for the difference overlaps zero, so the results are not statistically significant and could easily be due to chance.
Next Steps:
I will repeat the experiments, but measure blood pressure 5 times for each observation, increasing measurement precision.
For these experiments, I will test only 5 min. deep breathing and normal activity, but run 10 trials of each, with an interim analysis at 5 trials each.
Details
Purpose
To determine the effect of deep breathing protocols on short-term blood pressure.
All of these experiments were done before I tested the repeatability of my blood pressure meter and I only took one measurement per observation (i.e. one measurement before and one after each period). This was a big mistake on my part, as the variance between measurements was way to high and no results are statistically significant (i.e. could easily be due to chance).
Given this, please take all discussion/conclusions presented here as only suggestive for further experiments. I will be repeating this work with 5 measurements per observation.
Blood Pressure & Pulse Change during the Interventions
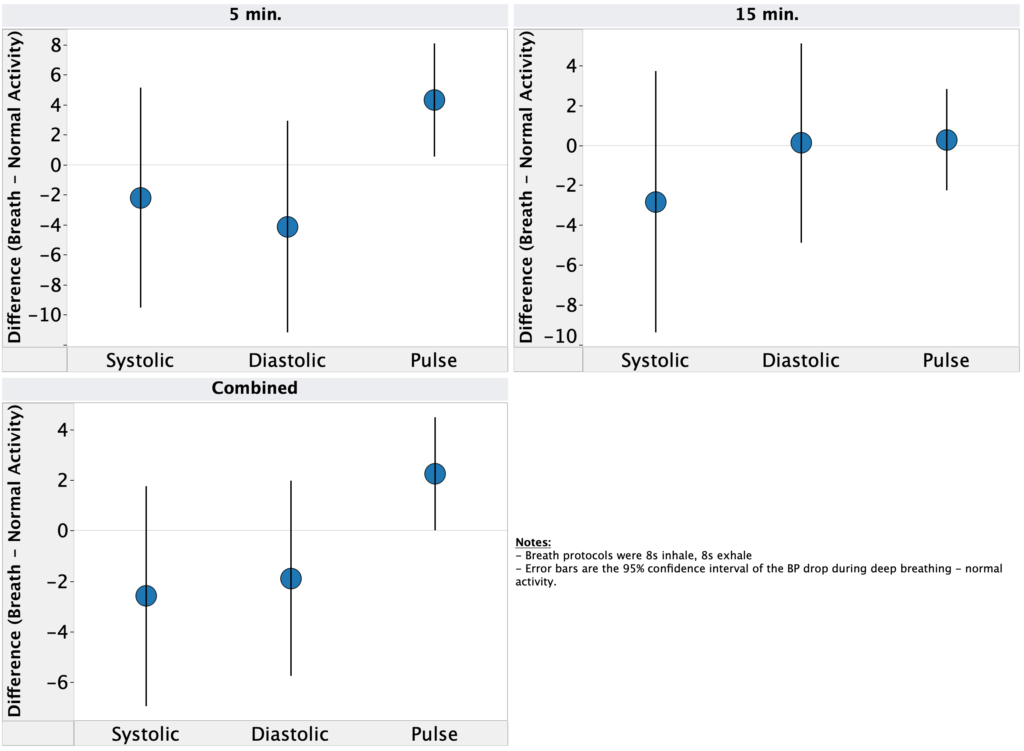
First, let’s take a look at the change in blood pressure during each session. As shown in both the table and graphs above, on average:
Systolic pressure dropped in both the 5 & 15 min. deep breathing conditions, while it increased during normal activity.
Diastolic pressure dropped in the 5 min. deep breathing condition, increased during 15 min., and increased in both times for normal activity
Pulse increased during 5 min. deep breathing, dropped during 15 min., and dropped in both times for normal activity
As discussed above, the 95% confidence interval overlaps zero for all of these measurements, so the results could easily be due to chance. However, they are consistent with my initial exploratory measurements.
Looking at the difference between means for each time condition, I see a drop of ~2.5 mmHg for systolic pressure, ~2 mmHg for diastolic, and an increase of ~2 bpm for pulse for deep breathing vs. normal activity. Again, 95% CI overlaps zero for all conditions, but the effect size is on the edge of worthwhile (I had pre-registered that I would follow up on effect sizes >3 mmHg).
Instead of using students t-test, I compared 95% confidence intervals between conditions (mathematically equivalent for a threshold of p = 0.05)
Blinding
This experiment was not blinded
Procedure
Each morning at ~6am, I measured my blood pressure before and after the following protocols:
8s inhale, 8s exhale, 5 min.
Normal activity, 5 min.
8s inhale, 8s exhale, 15 min.
Normal activity, 15 min.
Breath timing was controlled using the iBreath app.
Blood pressure measurements were performed using an Omron Evolve blood pressure meter.
For each measurement, I placed the meter on my left arm, ~4 cm above my elbow. Measurements were taken seated, with my feet on the ground and arms resting on a flat surface at a comfortable height (same every time).